

Abstract
Background:
Non-Hodgkin's Lymphoma (NHL) comprises a diverse group of malignancies with varied presentations and clinical behavior. Different prognostic factors have been defined including age, LDH, gender, CNS involvement and molecular/genetic characteristics. We aim to study the incidence and impact of skin involvement as a secondary site in patients with mature B and T-cell NHLs.
Methods:
The Surveillance, Epidemiology and End Results (SEER) database was used to identify patients (≥18 years) diagnosed with mature B/T/NK-cell NHL with skin as secondary site of involvement between 1973 and 2014. B-cell and T-cell lymphomas of all stages were included. Overall survival (OS) was estimated using the Kaplan-Meier method, and compared using Log-Rank test.
Results:
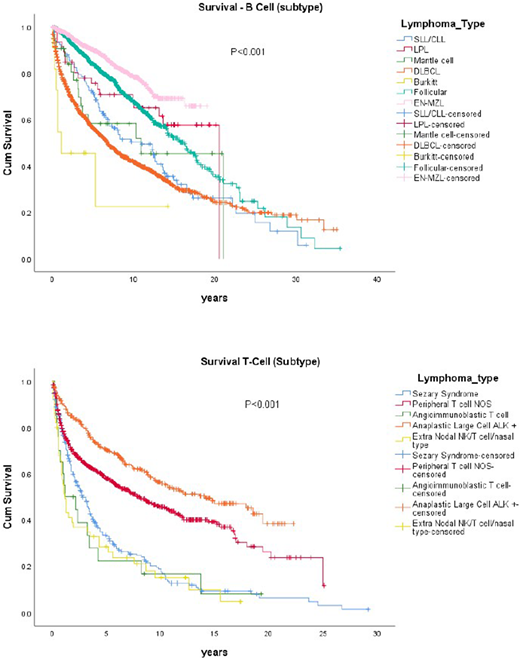
Total of 6429 patients were included with secondary skin involvement. B-cell NHL was more common with 76%. Median age for B-cell and T-cell NHL was 65 years (48-82), and 64 years (46-82), respectively. Slight male preponderance was noted in both subtypes (B-cell-56.7%% and T-cell-61.7%). Diffuse large B cell lymphoma (DLBCL) was the most common histology among B-cell NHLs, (DLBCL, N=1920 39.6%), followed by follicular (FL, N=1381, 28.5%) and extra nodal marginal zone (EN MZL, N=1314, 27.1%) Among T cell NHL histologies, peripheral T-cell NOS was the most common (PTCL, N=819, 51.6%) followed by anaplastic large cell ALK+ (ALCL+, N=341, 21.5%), and Sezary syndrome (N=293, 18.5%) Median overall survival was 6.1 [5.2 - 7.2.; 95% CI] years in T-cell population compared to B-cell population which was 13.3 [12.6-14.0; 95% CI] years. Survival was different by histologic subtype and correlated with SEER database relative survival for the overall population described in the SEER Cancer Statistics Review 1973-2011.
Conclusion:-
Skin involvement is relatively common in both B and T-cell NHLs. DLBCL, FL, MZL, PTCL-NOS and ALCL+ are the more commonly involved subtypes, correlating with their relative incidences. Outcomes in patients with secondary skin involvement tends to mimic known survival patterns in different histological subtypes conferring no additional prognostic significance. Skin as an extra nodal site of involvement should not change management for these patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal